VIBRATIONAL VIRTUAL BIOPSY
Increased tissue stiffness has been shown to be a characteristic of potential tumor metastasis and is the result of the abnormal deposition of collagen fibers.
Conventionally in order to confirm a diagnosis of cancer, a tissue biopsy is performed.
Biopsies:
- Invasive, expensive, time consuming (1 – 72 hours) & patient “unfriendly”
- It define lesion margins and depth but Ignores tissue stiffness (associated with various cancers and metastatic potential)
Vibrational Virtual Biopsies conducted with the help of VOCT are expected to be:
- More accurate
- Faster – 10 minutes
- Determine margins and depth and measures tissue stiffness
Vibrational OCT does for Dermatology and Mohs Surgery what MRI, X-ray and Ultrasound did for Radiology
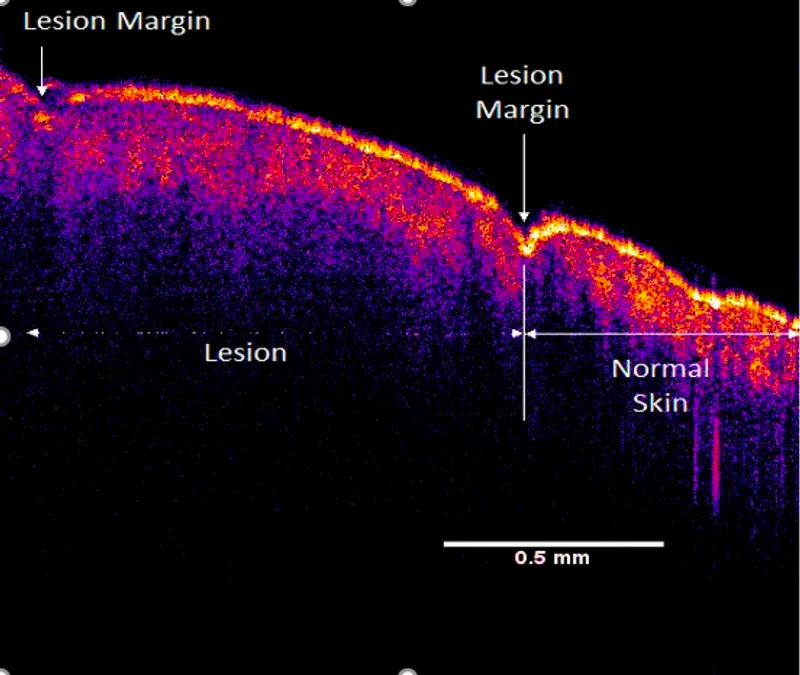
Enhanced OCT Image of scar (lesion) and normal skin using the Vibrational OptoScope
HOW IS THE “VIBRATIONAL VIRTUAL BIOPSY” USED TO DIFFERENTIATE BETWEEN BENIGN AND MALIGNANT SKIN LESIONS?

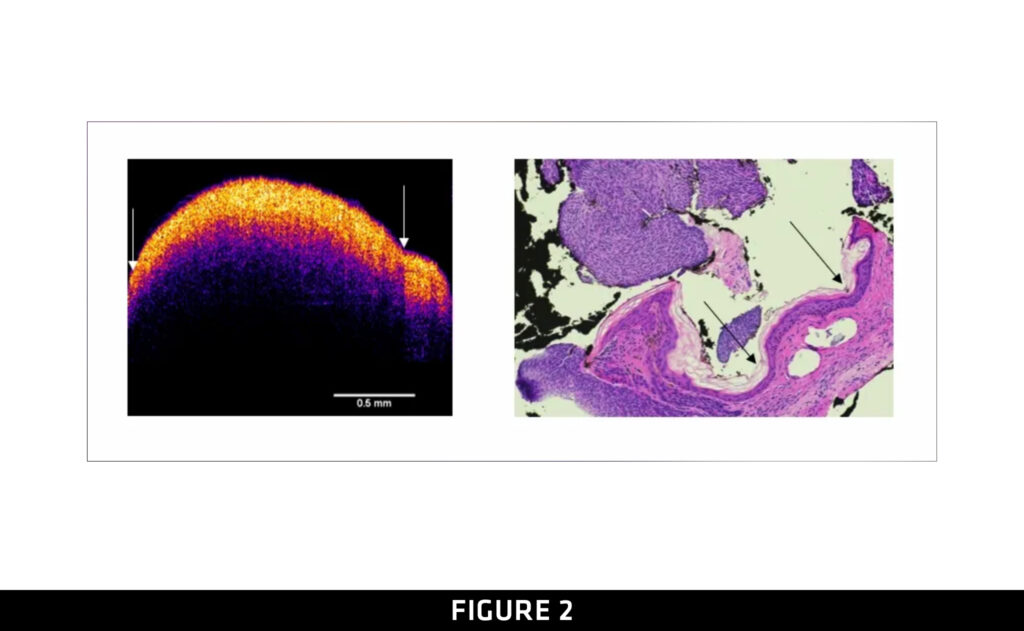
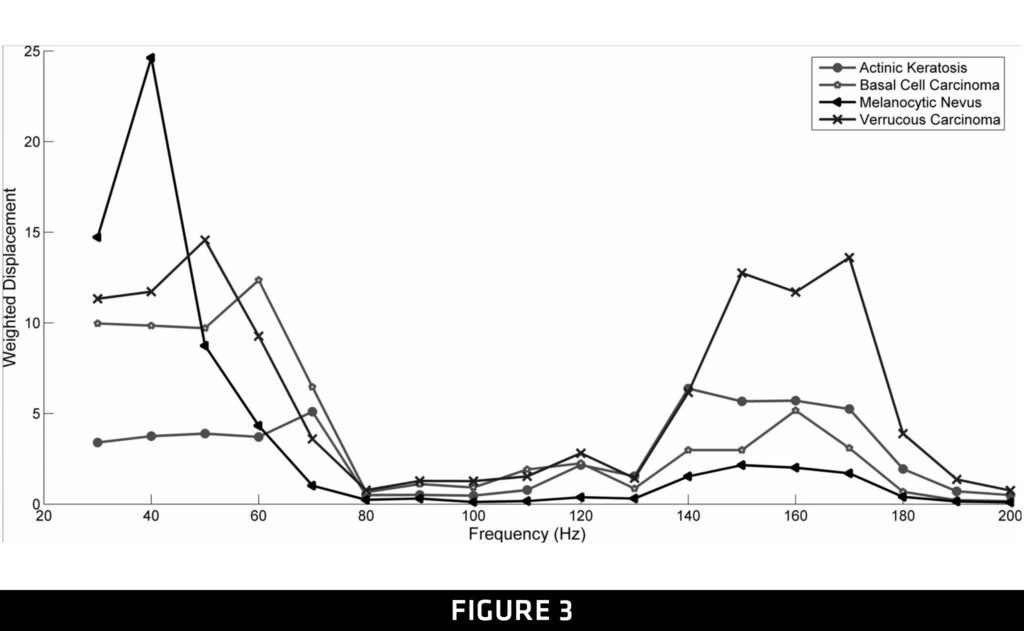
Figure 1. Weighted displacement for normal skin on left and scar tissue on the right.
Figure 2. On the left, OCT image for malignant basal cell carcinoma. On the right histopathology of the same malignant basal cell carcinoma.
Figure 3. Resonant frequency peaks for different skin lesions. Note the sharpness of the Melanocytic nevus epidermal peak at about 40 Hz (benign lesion) and the broadening of the basal cell and verrucous carcinoma peaks with malignancy.
Once the image and vibrational modulus is obtained from different lesions, the data can be compared to standard measurements on normal skin and benign and malignant skin lesions as shown in Figures 1 through 3. Normal skin has a very thin epidermis and has only one resonant frequency that reflects the collagen component as illustrated in Figure 1 . Benign lesions have two resonant frequencies, one from the thickened epidermis that is at about 40 Hz for the epidermis and one at 140 to 160 Hz that represents the collagen component as shown in Figure 2. Malignant lesions have two resonant frequencies; the epidermal peak is broadened and shifted to the left which the collagen peak is broadened (Figure 3). The shifting of the epidermal peak and its broadening is a characteristic “Finger Print” of malignant lesions.